
As I’ve said before, I believe the best birth plan, is no birth plan, but an informed pregnancy – that way, you can know your options, and can tackle whatever happens as it comes.
When you’re pregnant, there are a lot of firsts and a lot of unknowns. One area in particular that women build fear and anxiety around is labour….you don’t know the extent of the pain, or how you will cope with the pain. Interestingly, pain in labour can vary, due to environment, support people (a few tips here), whether labour is spontaneous or induced and whether you’re a first time mama or not. The more you fight the pain, the worse it hurts (increasing adrenaline and decreasing oxytocin) so giving into the pain and knowing that with every contraction you’re one closer (as corny and lame as it sounds) can help in relieving pain.
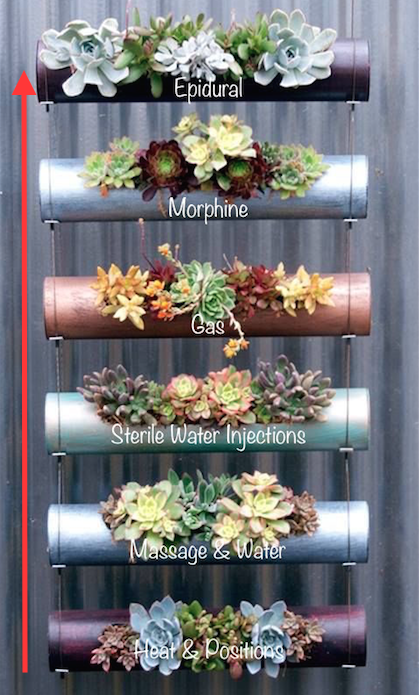
75% of women use some sort of pharmacological pain relief in labour, however there are non-pharmacological options available as well, so knowing what is available, is important. Below is our “pain relief ladder”, working our way up the ladder from natural pain relief to the big guns – we’ll explain each briefly and it’s effect on both mum/and or bub.
It is important to remember, you are free to choose whatever pain relief you want – it’s your labour, body and baby. The ladder works well in a sense that for women wanting as natural a birth as possible, it allows you to incrementally increase pain relief. Speak to your midwife/obstetrician antenatally more to gain greater insight into your options.
Breathing, Heat and Positions

How to use it?
– Heat packs (lower back, above pubic bone)
– Positions – staying active in birth is important. Gravity helps bring bub down, and helps to relieve pain and pressure, so rocking on a pregnancy ball, walking, sitting, all fours, lying on your left hand side, can help.
Safe for mum and baby?
-Yes!
Latest evidence
– According to recent research undertaken in NSW & QLD, Australia, it looked at the impact pharmacological and non-pharmacological pain relief had on labour outcomes (1835 women – link to paper at bottom of blog):
Extract from article: “Women who used breathing techniques were more likely to have a vaginal tear, forceps/ventouse suction, initiate breast-feeding, and continue breast-feeding beyond six weeks, compared to women who did not use breathing techniques.
The women who used breathing techniques were also less likely to have their baby admitted to a special care nursery.
Massage and Water
How to use it?
– Get the support person to massage any niggles with or without oil…your choice (many birthing suites had massage oil provided)
– Hop in the bath, or shower

Safe for mum and baby?
– Yes!
Latest evidence
Extract: “Women who used massage were more likely to have a vaginal tear, forceps/ventouse suction, initiate breast-feeding, and continue breast-feeding beyond six weeks, compared to women who did not use massage.
Women who used bath/birthing pool/shower were more likely to have a vaginal tear, and continue breast-feeding beyond six weeks, compared to women who did not use a bath/birthing pool/shower.
The women who used bath/birthing pool/shower were also less likely to have their baby admitted to a special care nursery.”
Sterile Water Injections

How to use it?
This is great for persistent lower back pain. Usually injections are given in four different places in your lower back, by two midwives, just beneath the skin, raising little blips on the skin. The injections really hurt! Like a strong bee sting, but this disappears after 30 seconds. The injections can bring up to two hours of pain relief to your lower back but you will still feel the contractions, the beauty of these are that, you an have them again at any time if they wear off, as it’s only sterile water.
Safe for mum and baby?
-Yes (cannot massage where the injections were as this can make them ineffective)
Laughing Gas (Nitrous Oxide) – approximately 50% of women utilise gas
How to use it?
Administered through a nozzle/whistle mouthpiece that you breathe in and out through, with the Nitrous Oxide and Oxygen being blended (able to be increased or decreased to effect). Nitrous Oxide very quickly enters the blood stream and takes approximately 15 seconds to kick in and 15 seconds to wear off….so you begin breathing as the pain is building and cease when the contraction has gone away.
Tip: try to keep your eyes closed as you’re using the gas…it makes you feel light headed and a bit dizzy, and then the room won’t spin as much!
Safe for mum and baby?
– Yes. Nitrous oxide does cross the placenta, however doesn’t leave by-products as it isn’t broken down by the liver, like drugs such as pethidine. It is quickly eliminated from the woman’s body and from bub’s.
Evidence
Extract: “Women who required gas were more likely to have a vaginal tear and forceps/ventouse suction, compared to women who did not require gas. The women who required gas were also less likely to have their baby admitted to a special care nursery.”
Side Effects
– Laughing gas can make some women dizzy, nauseous and/or vomit. Some may not find it effective pain relief.
Morphine (systemic opioids) – approximately 22% of women use systemic opioids
How to use it?
Injection given by a healthcare professional, taking approximately 20 minutes to feel the effects of the drug.
Safe for mum and baby?
Morphine does cross the placenta, and if bub is birthed within 4 hours of the injection, they can be a little bit more drowsy than babies of women that hadn’t had opioids. Dependent on hospital policy, a paediatrician may then be present for the birth.
Evidence
Extract: “Women who used pethidine were more likely to have forceps/ventouse suction (p=0.002) and less likely to continue breast-feeding beyond six weeks (p=0.03), compared to women who did not require pethidine.”
NB: This extract specificially looked at pethidine and not morphine, however I have still included the data for an opioid reference. Morphine competes for the same central nervous system receptors that pethidine does, however they are not the same!
Epidural – approximately 29.7% of women receive an epidural
How to use it?
Anaesthetist will be present to insert the epidural catheter into the epidural space in your spine. Link here to read more about epidurals. You will lose sensation from your waist down, dependent of the efficacy of the block, and therefore will have a indwelling urinary catheter inserted and be in the bed.
Safe for mum and baby?
Click here
Evidence
-Extract “Women who required an epidural were more likely to have forceps/ventouse suction and have their baby admitted to a special care nursery, compared to women who did not require an epidural. The women who used epidural were also less likely to have a vaginal tear and less likely to continue breast-feeding beyond six weeks. In contrast, women who required an epidural were 3.38 times more likely to have their baby admitted to special care, compared to women who did not require an epidural.”
Resources:
Adams, J., Frawley, J., Steel, A., Broom, A. & Sibbritt, D. 2015, ‘Use of pharmacological and non-pharmacological labour pain management techniques and their relationship to maternal and infant birth outcomes: Examination of a nationally representative sample of 1835 pregnant women’, Journal of Midwifery, vol 31 (458-463).


One thought on “The childbirth pain relief ladder”