Anecdotally when speaking with women about childbirth, in a professional setting or with girlfriends one fear brought up commonly is “I’m worried about tearing”. Now this is a totally valid feeling and fear, however this information should help you to understand how incredibly common (and often not that big of a deal) peri tears are.
Current research have the odds of sustaining a peri tear at around 85% (with the majority being low grade tears (defined below) and 0.6%-11% being the more severe ones (defined below).
In my opinion, women should head into labour not wanting to not tear (although, that is the ideal) but armed with the tools to best help minimise tearing and understand how best to manage and heal post birth.
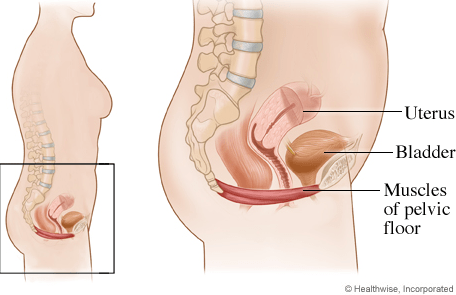
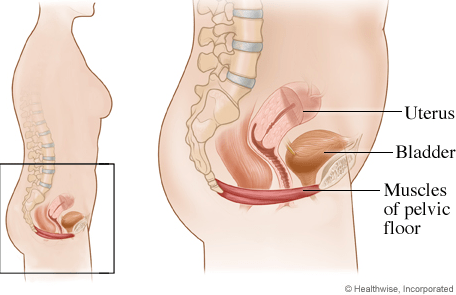
What is the perineum? Where is the perineum?
The perineum is the area shaped like a diamond, that involves your vagina and anus. It involves the superficial and deep structures of that region.
What are the stats around tears?
The more babies you have the incidence of peri tears decreases. Perineal tears reduce from 90.4% in women who are first time mamas to 68.8% in women who are having subsequent babies.
Are there risk factors to perineal tearing?
Yes. There are maternal, baby and intrapartum risk factors to consider. The factors greatest in your control (remember birth is unpredictable and birth plans sometimes should be seen more as birth wishes…have your ideal plan A but also be open to B and C) are the intrapartum risk factors. These are the things that you can do during labour and birth to help minimise tearing.
Some of these risk factors (but not limited to) include:
- epidural use (as this greatly restricts your movement)
- use of oxytocin (statistically intervention leads to more intervention)
- instrumental birth (vacuum or forceps)
- episiotomy
- prolonged second stage (>60 mins)
** the research within this study didn’t indicate whether this 60 minutes was a blanketed time for both first time mothers and/or mums of multiple babies. Some studies give first time mothers a longer second stage before considering it “prolonged”.**
Questions to discuss with your health practitioner antenatally?
- Discuss what your hospital or care providers vaginal examination policy is.
- Discuss birthing positions, use of water (does the hospital offer warm compresses?)
- Discuss perineal massage antenatally and have a discussion around whether this is something that could be beneficial for you (we have a free how-to download here).
Grades of tearing?
Perineal tears are graded from a labial graze and then one to four.
The most common are labial grazes, 1st degree tears (shallow tear to the skin) and 2nd degree tears (tear to the skin and muscle).
3rd (3A,3B,3C) degree and 4th degree tears are not as common (these all vary in definition, but to keep it simple they involve a tear to the skin, perineal muscle, and/or internal and external anal sphincter muscles — a 4th degree tear, involves a tear into the anal sphincter.
What’s the latest evidence saying?
- Current evidence published in 2020 (Pubmed), retrospectively studied 22,387 pregnant women, and looked at the association between the number of vaginal examinations during labour and perineal trauma. The study concluded that performing five or more vaginal examinations (VEs) during active labour is associated with an increased risk of severe perineal trauma (defined as grade 3-4). [DOI: 10.1007/s00404-020-05552-z]
- Lying on your side, kneeling, standing or being on your hands and knees when you give birth will help. If you want more info on birth positions, head over here and have a read.
- Avoiding long stretches of time squatting, sitting, or using a birth stool when you are pushing – if you’re getting good comfort from these positions, just switch it up, rotate your way through.
- Ask your midwife to hold a warm, wet compress (a sterile hospital washcloth) on your perineum while you are pushing. Research concluded from a randomised control trial looking at the efficacy of warm peri compresses whilst pushing that women reported less pain whilst pushing when using a warm compress, working as a pain relief.
‘The use of a warm of a warm pack failed to decrease the likelihood of a laceration requiring sutures, which occurred in about 80% of women in both groups…however…women (who didn’t receive warm compresses) were more than twice as likely to have an anal tear (8.7% vs. 4.2%)’. – Dahlen et al.
It also was linked to less perineal pain in the days after birth, as well as less reported urinary incontinence reported three months post birth.
Healing after birth
- Make sure your sutures are looked at by a health professional
- Keep clean and dry
- Use ice and pain relief to minimise swelling
- Begin pelvic floor exercises as soon as possible in the days post birth
- If you sustain a more substantial tear, it’s important to follow up and be referred onto a physio that specialises in women’s health.
- If in doubt, and you have questions, speak to your midwife, obstetrician, or GP.
Continue reading “A Birth Fear Explained; The Peri Tear – Latest Evidence”