Anyone that’s had a baby, or watched “Call the Midwife” or “One born every minute” knows birth is messy…and when we say messy we mean that you don’t labour in your Camilla … there’s fluid, it’s primal, innate and magical all in one! And amongst all the vernix, amniotic fluid and blood, are microbes (good bugs), which babies born vaginally are exposed to whilst making their way through the birth canal.
This exposure to approximately 300 ‘good bugs’ from the birth canal helps to build a child’s microbiome (the army of bugs that protects us from germs, breaks down food for energy, etc.).
But what happens if you don’t have a vaginal birth, and have a caesarean? – Does this mean bub misses out on these good bugs?
Not anymore! Let’s talk seeding…
With one in three bubbas being born in Australia via caesarean, and by bypassing the birth canal, it means that they are therefore not exposed to the bugs, which is leading to the ongoing research debating the lower levels of autoimmunity of bubs born by caesar. So it’s great to hear that there are now methods out there for littlies to receive these good bugs regardless, hopefully increasing immunity for all! (Research is still pending on the efficacy of this in comparison to vaginal birth…but it can’t hurt, right?)
How is seeding done?
Seeding is carried out by inserting a sterile swab into the vagina (like a tampon), leaving it there for a little bit to absorb, then giving it a swirl and taking it out. When bub is born, this swab is put in your baby’s mouth and wiped across their little body immediately, trying to emulate a vaginal birth.
If this is something that’s of interest to you, please discuss it with your midwife or obstetrician, especially if you know you’re having a caesarean for whatever reason or thinking of going down the VBAC road.
References and Articles: (to come!)
Image via janabrasilfotografia and @birthwithoutfear
It’s plays one of the most important roles throughout pregnancy and then we chuck it?! What you could do with it, if you were to keep it…
Over the past 24 hours, the placenta (the organ that nourishes and oxygenates the baby whilst in utero) has been a talking point on social media. A photo published by a Brisbane photographer on Facebook (and Insty) (here) showed a little bubba still attached to the placenta, and the Maori traditions that would be practiced postnatally by his family. Which got me thinking…if this photo has received such broad recognition over something that I thought was known information, maybe the placenta and what happens to it afterwards, or ways to treasure it aren’t known?!
Let’s rewind briefly…the placenta is the huge bed of blood vessels that begins developing at implantation and imbeds itself into the uterine lining, with the umbilical cord stemming from here. Most commonly the placenta will attach to the top of side of the uterus – if you want to know where yours is out of curiosity, ask the sonographer at your next scan.
The health of your placenta is a result of lifestyle, age, nutrition, health (blood pressure, blood clotting disorders, substance abuse, smoking), etc.
After the birth of a baby, the placenta follows suit either physiologically or managed actively. Physiological management of the third stage is where the midwife and mother wait for the placenta to naturally come away from the lining of the uterus. This is method should be discussed with your midwife or doctor as there are contraindications. If you do intend to birth the placenta physiologically, a strong focus on initiating breastfeeding and skin-to-skin with baby has been documented to encourage this separation.
The other method of placental delivery is through active management (this is what is most common and implemented in Australia); whereby a mother receives an intramuscular injection with consent of a synthetic oxytocic hormone to help contract the uterus and clamp down the blood vessels…encouraging separation and minimising blood loss immediately after birth. This is the same drug that is utilised in inductions of labour to make a uterus contract.
From here the placenta, the membranes and the umbilical cord are inspected by a midwife. Unless otherwise indicated (by certain factors throughout pregnancy, birth or birth outcome) the placenta will be discarded, unless the parents want to keep it*.
*This may be something to consider antenatally if you’re thinking about going down this road. From my contact with a few hospitals, I know that they will not keep your placenta refrigerated for you whilst you are at the hospital, so organising a way in which to get it home, and keep it refrigerated until you’re ready to carry out whatever you see fit, is worth a little advanced planning.
So for anyone wanting to somehow use or honour the placenta (I’m aware of how hippy dippy this sounds, but I couldn’t think of another word) here are a few to consider:
Lotus Birth is where the placenta is left attached to the baby at birth until the cord falls off on its own. Sometimes being covered with salts, herbs (rosemary and sage are often used), the placenta is then wrapped up, nappy style, so it’s not intrusive (or offensive) to some guests that may want a snuggle with bub. This is the downside to a lotus birth – so both partners need to be on board with the process for it to not hinder physical interaction with bub.
Placenta Encapsulation is when the placenta is steamed and cooked at a low temperature, dried and encapsulated into what look like ground vitamins. They are tasteless and are a way of receiving nutrients that have been suggested to:
-Help balance your hormones
-Replenish depleted iron levels
-Assist involution (the uterus returning to its pre-pregnant state over the 6 weeks post birth)
-Reduce postnatal bleeding
-Increase milk production
-Decrease the chances of postpartum depression
After speaking to other midwives one shift, a few stressed the importance of seeking out well practiced and known placental encapsulators. So, make sure you do your research beforehand and be sure to ask questions about the conditions and hygienic methods implemented throughout the process. Websites like, http://www.placentaservices.com.au/new-south-wales.html, work as directories for verified service providers.
image via placentanetwork.com
Placental Burial is the burial of the placenta under a tree or in a garden. The nutrients of the placenta are said by green thumbs to make a great fertilizer too, which is a bonus! If you do intend to plant it in the garden, make sure you bury it deep in the ground…no one wants an animal on the hunt for it…not good, not good! Also, if you’re worried that you may end up moving one day, it can always be planted in a large pot. That way the placental plant can move with you.
image via lisamckaywriting.com
Placenta Piccie – The name says it all really. Paint and dye are used to highlight the blood vessels to be printed onto paper. A keepsake that can be as colourful or monochromatic as you see fit.
image via shaunaowensphotography.com
In all it’s glory! Image via Pinterest
What did you do with your placenta? Was it trash or treasure? x
There’s been lots of VBAC discussion on our Instagram feed over the past couple of days. I wanted to have a greater handle on the recent facts and stats, so I was read an article on The Conversation by Hannah Dahlen last night on vaginal births after caesarean sections (VBAC) (read it here).
With nearly one in three women in Australia giving birth via caesarean, I feel like I am only really just now starting to hear more and more about VBAC’s. Yes, as Midwives we are taught and study this but anecdotally I hadn’t come in contact with many women asking for a VBAC, but more so of midwives asking women if they knew about a VBAC being an option and did they want to consider it.
It’s lovely to hear more women, through the channels and power of social media discussing topics like this, sharing birth stories and channelling positive empowering pregnancy energy.
It is important to mention that “most Australian women (84.4%) have a caesarean for subsequent births after a caesarean. Only 15.5% of women have a VBAC. In private hospitals, this rate is even lower, at 11% “(Hannah Dahlen)… however of the women that do attempt a VBAC, 70% of these women are successful in giving birth vaginally and do not need a repeat caesarean section. Which is nothing to sneeze at, right?
Yes, a repeat caesarean section is a decision that is solely that of the couple after an informed conversation with their health practitioner, and fabulous advancements in research now mean that babies are not separated from their mamas (health of mum and bub permitting) and there are things like seeding available for women (vaginal microbes wiped onto babies as they are born via caesarean so to simulate as best possible the antimicrobial goodness bubs receive from the birth canal) and skin-to-skin and breastfeeding support happening in theatres and recovery; facilitating the mother-infant dyad.
But if you’re a low risk, healthy mama, and want the option of a VBAC, and want to know more, continue reading!
It’s a conversation worth having antenatally with your midwife or obstetrician!
Benefits of a VBAC?
Greater chance of uncomplicated births in the future
Recovery is a lot quicker – due to no abdominal surgery
Reduced risk of blot clots
Skin-to-skin, mother-infant bonding, breastfeeding etc. may be established quicker.
Shorter stay in hospital
Risks of a VBAC?
uterine rupture may occur. Statistics are about 1 in 200 VBAC’s there will be a uterine rupture (the scale of which varies drastically from slight rupture to the uterus opening up completely…which is very much cause for concern and can have dire outcomes).
“In terms of the baby’s safety, guidelines on VBAC just released by the United Kingdom’s Royal College of Obstetricians and Gynaecologists (RCOG) state that the risk of a baby dying during labour and birth is extremely low and is similar to the risk for women having their first baby”(Hannah Dahlen).
Do VBAC outcomes differ based on hospital setting?
Some hospitals in Australia offer VBAC programs for mothers that have had 1 caesarean section…other hospitals have programs that offer women the option of a VBAC after 2 caesarean sections.
Does a VBAC mean I have to labour differently?
Continuous cardiotocograph monitoring (CTG) may be implemented to keep a close eye of the wellbeing of bub. Protocols may vary from hospital, state, obstetrician etc., so this is a good question to ask your midwife of doctor so you know what to expect.
So if you’ve had a previous caesarean section and are unsure as to your personal situation and your options, asking lots of questions to you midwife or obstetrician, and regardless of whether you choose to try for a VBAC or choose an elective caesarean, just asking questions helps to make informed decisions.
Image via Hannah Tallo of a VBAC mama
Resource: hyperlinked article (first paragraph) The Conversation, Hannah Dahlen
Language carries weight and power. We have a question for you…
It could be argued that the time in a woman’s life where she will seek, question and be influenced by information the most is during pregnancy. Pepper in hormones, lack of sleep and a tiny touch of anxiety about the impending birth and you have a woman that is susceptible to the weight and power of language.
We know that words have the ability to empower us, and also destroy our confidence. Statistically, we are more likely to say stuff we regret or that might be less thought out when we are under pressure, feel out of our depth, are in an unfamiliar environment or anxious (welcome to a birthing room).
As midwives throughout our training we focus on woman-centred language, and ways in which to support and empower women giving birth, including ways in which to make the birthing environment feel safe and reassuring. This is all well and good, but reassurance from a loved one, and/or support partner is invaluable, and may hold more weight physically and emotionally for some women.
So….we’re throwing this one out to you guys….what words of empowerment; from either your midwife, doula, obstetrician, loved one, or support partner, got you across the line? What do you remember most vividly? Keeping in mind that language is not always verbal. Physical language is also telling.
Sharing is caring! We’d love for you to comment below (short and sweet, or long and lengthy, you pick) and share in the positivity and empowerment of birthing language.
For all the lovebirds contemplating or expecting a bub next year, have a squiz at the Chinese gender calendar. Are you having a boy or a girl?
Just a quick shoutout to all the gorgeous peeps that have been along for the Winnie Wagtail ride for the past 5 months. We’re thrilled the whirlwind that was 2015 is coming to an end and can’t wait for 2016!
Whilst we contemplate New Years resolutions, and get stuck into the bubbly, for all the lovebirds contemplating a bub for next year (the year of the monkey) have a squiz at the Chinese gender calendar. This is not evidence-based, but said to have been discovered in a tomb over 700 years ago, it is supposedly over 90% accurate. My husband and I backtracked friends, family and siblings, and only twice was it incorrect from our experience. It’s a bit of fun for guessing your baby’s gender, or planning ahead (with 50/50 odds, and this supposedly higher, you can’t really go wrong!)
Kim Kardashian-West brought breech babies into the spotlight recently…here’s the 411 on ECV’s and what you need to know
As I’m sure your social media feed has already informed you, Kimye have welcomed their second bub, a baby boy named Saint.
A couple of weeks ago a mum-friendly website posted an article, “Kim Kardashian’s baby is no longer breech after a “painful and scary” medical procedure”, (read it here). It was admittedly 95% Kim’s words extracted from her website about having a breech baby and attempting to turn the baby externally, through what is called an ECV (External Cephalic Version).
Kim goes on to explain how ‘she was prepared for an emergency caesarean…her waters could break… and that it was more painful than childbirth as she wasn’t given drugs.’
I believe this article missed an opportunity in this article to explain; What an ECV is? What are the risks? What is the success rate? Can you use pain relief? Are their alternative remedies or avenues available to explore for turning a baby from a breech position to a cephalic position (head down)?
Of course by Kim Kardashian-West publishing her experience (as is her right), and the media reinforcing it without a counter argument, or without any evidence-based research to back up what she is saying, I believe this is doing women (who may find the whole childbirth thing scary enough as it is) a disservice.
So below we’re breaking down what is an ECV with some evidence based research (we can’t promise it’ll be as entertaining and dramatic!):
What is Breech? Breech is the name given to a baby that is head up, bottom (or feet) down towards the vagina. This accounts for approximately 3-4% of pregnancies. This fetal position is regarded as higher risk for the baby regardless of the mode of birth (Cochrane Review 2015).
Image via nlm.nih.gov/medlineplus
What is an ECV? External Cephalic Version aims to turn the baby from a breech position to a cephalic position, by pressing gently on the mothers stomach.
Andrew Bisits is the Director of Obstetrics at the Royal Hospital for Women, Sydney, Australia – a tertiary academic hospital which oversees 4000 births per year. He’s been in obstetrics for 30 years and has a strong interest in breech pregnancies and vaginal breech birth.
Below is Andrew Bisits performing an ECV:
Who performs an ECV?
Obstetrician’s perform ECVs. This is not under a midwives scope of practice in Australia.
What are the risks?
An excerpt from the Cochrane Review 2015, External cephalic version for breech presentation before term (review), concluded that ‘comparedwithnoECVattempt, anECVcommencedbeforetermimproves cephalic presentation (head down)atbirth.Beginning anECVbetween34to35weeksmayhavesomebenefitintermsofdecreasingtherateofnon-cephalicpresentation (babies not head down), andriskofvaginalbreechbirth. An earlyECVmayincrease the riskoflatepretermbirth.’
The review also highlights the importance ofcarefuldiscussionwithwomenaboutthetiming of an ECV so that informed decisions can be made.
The overall complication rate of ECV’s according to evidencebasedbirth.com was 6%, and the rate of serious complications (placenta abruption or stillbirth) was 0.24%
What is the success rate of turning bubs?
According to BabyCenter the success rate of an ECV is 58%. If the baby is in a transverse lie (sideways), the success rate increases to 90%. This website also reported that the ECV was more likely to work if it wasn’t a woman’s first baby.
Can you use pain relief for the procedure?
Pain relief, such as nitrous oxide (happy gas) inhalation during the procedure decreases the level of ‘severe pain experienced by some women’ and appears to be safe for both mother and child, with no effect on the success rate of ECV or the perinatal outcomes (Burgos et al. 2013) – Source: nitrous oxide for analgesia in external cephalic version at term: prospective comparative study.
Having seen ECV’s performed, how uncomfortable a woman finds the procedure varies. Not everyone will find this more painful than childbirth, yes uncomfortable, but not traumatising pain. Talking about viability of using pain relief would be a question to ask your obstetrician before commencing the procedure.
Alternative methods for trying to turn babies?
Speak to your healthcare providers about the potential benefits of massage, acupuncture, swimming, positions etc.
Can I have a vaginal breech birth?
Vaginal breech birth has become a lost skill over the years, and many doctors will choose (and believe it safer) to perform as caesarean section. It is important to discuss the risks and your personal pregnancy situation with your healthcare provider, however there are some obstetricians that will support vaginal breech birth.
Can I opt for a caesarean section and not have an ECV?
Of course, it’s your pregnancy and your baby. This is also a good conversation to have with your obstetrician and midwives.
Evidence-based info for parents-to-be.
Follow us @winniewagtail
Do babies need water? Small boobs, no milk? We’re setting the record straight!
There are many myths out there surrounding breastfeeding. Some myths are passed down through generations, some specific to certain cultures, and of course, from mama-to-mama experience. Another factor is that with constant research being undertaken for greater evidence in pregnancy related areas, what we once did, may not be of best practice or recommended anymore. So here are some common questions/myths and their answers/debunking.
Q: It’s a hot day, so I’ll give my baby (<6months) a bottle of water?
A: No your little bubba does not need a bottle of water. Breastmilk has 2 parts (once the milk is in). Firstly when the baby latches it will suck more intensely and quickly…this is when the baby is getting foremilk, a thin, thirst quenching milk. When the baby switches rhythms and begins slower, more nutritive sucking, bub is receiving the hindmilk (a fattier, densely nutritious, calorie fuelled milk). So on a hot day, you might find your baby feeds more frequently and for short amounts of time…this is because baby is requiring the thirst quenching milk. Make sure you keep your own fluids up!
Q: I’ve got small boobs, so does that mean I don’t produce as much milk as someone with big boobs?
A: Breast size doesn’t affect milk production in the majority of women, this is because breast tissue is for the most part connective tissue and fatty tissue rather than milk producing glands. The amount of milk produced is connected to how often, how well and for how long bub feeds.
Q: My mother didn’t make much milk, so I won’t either:
A: Since your mum has had babies, a lot has changed. We now strongly encourage skin-to-skin immediately after birth (no washing of bub beforehand) and mother-infant bonding as well as rooming in with your baby. Complimentary feeds are not as frequent as they once were and many hospitals are striving for BFHI (Baby Friendly Hospital Initiative) accreditation which encourages breastfeeding and its benefits, and only utilising formula if there is a medical indication or maternal request.
Q: (Day 1) I don’t have enough milk:
A: When your baby is born and before your milk comes in around day 3-4, you have colostrum – a gold coloured, sticky fluid that your body has been making and storing since you were 16 weeks pregnant. Colostrum is not only gold in colour, it is liquid gold! It is densely rich in your antibodies, calories, protein and has a laxative effect (helping to push out the meconium, the black sticky poo, stimulating baby’s tummy) to make more room for breastmilk. You make the perfect amount of breastmilk for your baby. Colostrum is the initial breastmilk, and is of a lower volume than foremilk and hindmilk, however it is the perfect amount for your baby’s tiny tummy, at that point in time (see the image at the bottom of article).
Q: Formula fed babes are better sleepers than breastfed babes: A: Formula and breastmilk have a difference composition and different protein molecules. Formula has larger protein molecules, meaning that it takes the baby longer to process and metabolise…sitting in their tummy longer…keeping them fuller for longer. Research has shown that though formula fed babies may sleep for longer periods than breastfed babies, their sleep quality is not of a better quality.
Breastfed babies begin to sleep for longer periods from around 4-6 weeks and it is at this time that their sleep duration seems to equate to that of a formula-fed bub.
FYI – Why babies don’t need a crazy amount of breastmilk on Day 1, and why they want to feed constantly in the days to come is explained perfectly in this picture below. Babies have tiny tummies, and breastmilk is metabolised very easily and quickly…hence their frequent feeding. Babies also feed frequently because they’re clever and know this brings the milk in quicker, especially at night time in the early days. You breastmilk producing hormone, Prolactin, is highest at night…and babies know it…hence why they sleep more soundly during the day and are crazily feeding throughout the night. Hang in there – they won’t be possessed, breastmilk crazy night monsters for too long!
via Pinterest
Reference:
Saggy Boobs and Other Breastfeeding Myths 2008. Scotland. (This is an evidence based book that doesn’t take itself too seriously. An interesting read for mama’s wanting more info and more myths debunked!)
Birth isn’t always like the movies. We’re breaking down the stages of labour from the first niggling pains to the birth of the placenta.
A lot of people think that as soon as labour pains begin, you dash erratically screaming and speeding to the hospital, like what you see on the movies. No, no – for the most part, it’s not like that…
We’re breaking down the stages of labour from the first niggles to having bub in your arms to the birth of the placenta. Let’s begin*!
*(Pregnant mamas – get your support person/people to look at this timeline – it’s a great reference tool so that they understand what you’re experiencing, what they can do to support you and what the midwife will be doing along the way. Also get them to check out this article on ways to support you during labour and birth).
P.S. As much as I’d love to be able to predict date of births, time of births, and mode of births (I’d be a bagillionaire) I can’t. Every one is different, and every labour is different, so this is just a rough anecdotal guide to each stage.
P.P.S. We haven’t spoken about pain relief options throughout the stages, but there’s stacks of evidence based info on pain relief here.
P.P.P.S. Lastly, membranes can rupture at any point in the birthing process, so we’ve left them off the timeline, as there’s no telling when this will happen.
EARLY LABOUR
Physical Signs women may experience:
– Irregular niggling pains (like period cramps)
– Contractions can be irregular, regular or not even felt.
– Loose bowels
– Bloody show (mucous plug that falls away from the opening of the cervix) Emotions women may experience: – Maybe this is it!
– Q: Should I go to the hospital now? (A: Call and speak to a birthing unit midwife, and they will help you with a bit of a plan for when to come in/ when to call back)
– I’m not sure if this is labour or not?! Behaviour Anxious – lots of walking…talking…smiling…restless…excitable…hungry…may not want to talk when having a contraction.
This period can last days, and be on and off. Some women won’t even notice this phase. This is the time where cervical changes begins.
FIRST STAGE
Physical Signs women may experience:
– Pains are stronger, more regular
– May feel a pattern starting to emerge
– Talking through contractions is becoming more of an effort Emotions women may experience: – It’s happening!
– Committed to the process
– Confident…. “I can do it” Behaviour – Lots of position changing…figuring out what is working best as pain relief (article on pain relief) and for comfort.
-lots of walking
*Late first stage – women can become more insular…they’re working hard and have a ‘Shh, I’m working” attitude towards birth. They begin to close their eyes more. This is the time where women become less modest, and loose inhibition. They are starting to feel more tired and start talking about sleep and how tired they are.
TRANSITION
Contractions can become more painful and frequent on that home stretch to being fully dilated (10cms). This is the point in time where a woman may begin to self doubt, may become confused, scream, tell you “she’s dying”… “giving up”…”going home”…
Women can become shaky, nauseous, vomit…have the urge to go to the toilet, as bub moves down the birth canal…it really depends.
As weird as it sounds this is a good sign! It means labour has progressed and baby is much closer to arriving!
SECOND STAGE – this is the pushing phase
Physical Signs women may experience:
– Mucousy show
– A second burst of energy
– Urge to go to the loo
– Spontaneously pushing
* experience feelings of stretching, stinging, burning – all are common. Emotions women may experience: – More alert
– Chattier
– May be tired and sleep between contractions Behaviour – Calmer after transition
– Desire to focus so she can meet her baby
The birth of the placenta, can be either physiologically or actively managed (we will write a post on these modes of delivery soon!). Hopefully this will all be happening whilst you’re snuggling with your bub. Make sure you have a squiz at our article on delayed cord clamping – it’s a must read for mamas-to-be.
Because this isn’t the most evidence-based article we’ve written, here are some references so you can do some extra homework x
So many books, so little time! So here’s our top 5 pregnancy reads before bubs arrival.
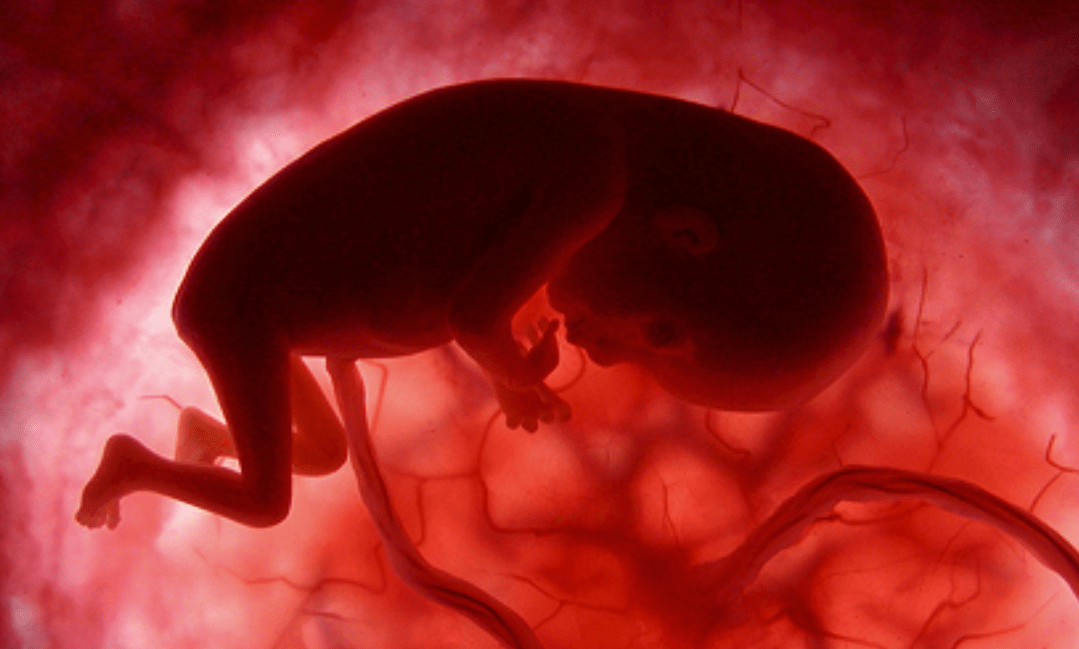
1. For great weekly pics and blurbs about baby’s development, our pic is an oldie but a goodie (be prepared for some serious 80s bush!)…Lennart Neilson’s ‘A child is born’. Originally published in 1965 it’s old, but the pics are fab!
2. A go-to reference for the early development in the early days of parenting. Dr. Howard Chilton provides information, that is evidence based. Simplistic and reassuring. A must-read!
3. Written by a woman known as ‘the mother of midwifery’, Ina May Gaskin shares her knowledge of natural birth. This isn’t a “hippy dippy, garden dancing” read. Spiritual Midwifery regales you with real birth stories that we can all learn from. Ina May shares techniques to get you through labour and birth, as well as understanding the mechanics of labour. Fabulous to get you confident about birth and ready to meet your bub!
4. Originally written in 1959, Childbirth without fear isn’t to be feared (unlike the front cover – not one for the bus!) Written by an old-school obstetrician, the wording can be technical at times (I just skipped over these parts!), but the information surrounding fear is fundamental. He explains the impact fear can play on the outcome of your labour and the importance of having the right people around you. It’s well worth having a squiz.
5.Written by a registered nurse / midwife / early childhood nurse with over 30 years, Baby Love, is a go-to. Simplistic, realistic and a great reference to have on the shelf – for everything from sleeping and crying to nutritious recipes.
Did you know that over 1000 new parents each week in Australia are diagnosed with PND? Know the signs and symptoms!
Did you know that over 1000 new parents each week in Australia are diagnosed with postnatal depression (PND)? It’s a devastating statistic, and a debilitating illness. PND is not culturally, age or gender bias; and both men and women can suffer from it mildly, moderately or severely, immediately after birth or gradually in the weeks, months and year after birth. It can rear its ugly head after miscarriage, stillbirth, normal births, traumatic births and caesarean sections.
It is normal and common for women around day 3 post birth to feel teary, irritable, overly sensitive and moody. This is due to a woman’s hormone levels yo-yoing all over the place…around the same time as the milk is coming in…(convenient, right?!). It is okay to feel like this on and off for a few days, but if it persists, seek support and help is a must.
In light of September bringing awareness to depression and suicide through R U OK Day and it being Suicide Prevention Month, we thought this was apt timing to bring awareness to this commonly fought illness.
It is important to remember that this is an illness and not a reflection on you personally or as a mother or father. There are ways through postnatal depression, and we’ve provided a list of some of the support avenues out there at the bottom of this post. It is imperative that you seek professional help – speak to your GP.
Signs and Symptoms
According to PANDA, The Perinatal Anxiety & Depression Australia organisation, a combination of the following symptoms for someone suffering from PND is not uncommon:
















 Evidence-based info for parents-to-be.
Follow us @winniewagtail
Evidence-based info for parents-to-be.
Follow us @winniewagtail